Intermittent fasting works differently at every age — and the LDL risk is real for all of them
Xing et al. (2026, Nutrients, 28 RCTs, N=1,833) is the largest age-stratified meta-analysis of IF to date. IF produces distinct metabolic trajectories by age group: adults 45+ gain the strongest cardiovascular benefits (−7.83 mg/dL TG, −4.86 mmHg SBP) but also face the most dangerous lean-mass risk. LDL-C rises at every age and across both TRF and IER protocols — making lipid monitoring a universal requirement. GRADE certainty is low to very low; article closes with concrete age-stratified dietary guidance including the authors' "IF+" protocol for adults 45+.

리서치 브리프
Intermittent fasting (IF) produces meaningful weight loss across every decade of adult life. That much is now well established. What a new systematic review and meta-analysis makes harder to ignore is the rest of the story: the metabolic trade-offs shift significantly by age, two specific risks appear in every age group, and the group that loses the most weight (adults 45 and older) faces the most clinically dangerous version of those risks.
Xing et al. (2026), published June 3 in Nutrients (MDPI, Q1, IF 5.0), pooled 28 randomized controlled trials involving 1,833 participants — the largest age-stratified meta-analysis of IF to date — and reported that IF elicits "distinct, age-specific metabolic trajectories" that challenge the standard practice of applying a single IF protocol to anyone who asks for one. 1
Study design
Study type: Systematic review and meta-analysis of parallel-group RCTs (pre-registered, PROSPERO CRD420251028745) · Journal: Nutrients (MDPI, Volume 18, Issue 11, Article 1799) · Published: June 3, 2026 · Peer-review status: Published, open access (CC BY 4.0)
All ten authors are affiliated with the School of Public Health, Ningxia Medical University, Yinchuan, China. Funding came from the National Natural Science Foundation of China and a Danone Institute research grant; no conflicts of interest were declared. 1
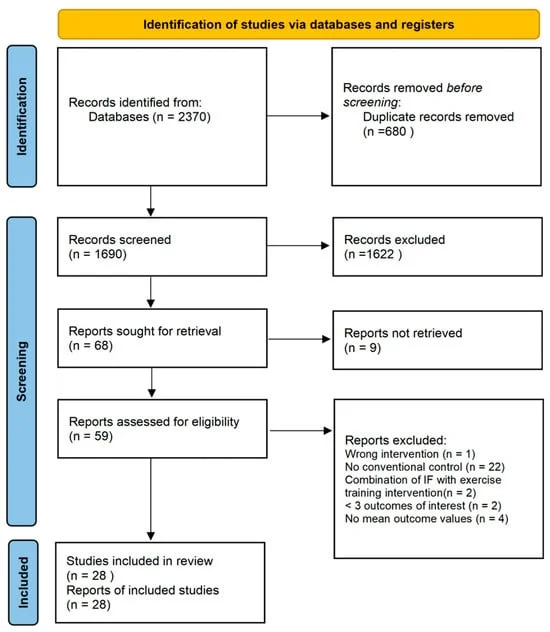
Xing et al. searched PubMed, Scopus, and Web of Science from inception through September 2025. From 2,370 records, 680 duplicates were removed, leaving 1,690 titles and abstracts to screen. Fifty-nine full texts were assessed for eligibility; 31 were excluded. The final pool was 28 parallel-group RCTs with a combined 1,833 participants, age range 21–70 years, BMI range 20.3–38.0 kg/m². 1
Intervention: Time-restricted feeding (TRF) in 19 studies, alternate-day fasting (ADF) in 7, and the 5:2 diet in 2. Control was habitual or ad libitum diet. Trial durations ran from 4 weeks to 12 months. Participants were healthy adults, or adults with overweight or obesity, without pre-existing diabetes, cardiovascular disease, or metabolic syndrome.
Analysis: Random-effects model, effect size expressed as mean difference (MD) with 95% CI. Heterogeneity reported as I². A conservative sensitivity analysis used a correlation coefficient of r = 0.5 (vs. the standard r = 0.8 default) to avoid artificially narrow confidence intervals. Leave-one-out sensitivity analyses were run on all outcomes. GRADE certainty was assessed for every outcome.
What changes with age
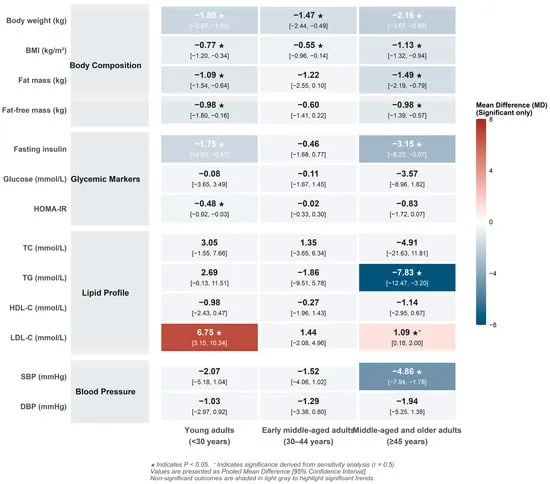
The authors divided participants into three strata using study-level mean age: under 30, 30–44, and 45 and older. Results across 13 outcomes differed enough between strata to matter clinically.
| Outcome | Under 30 | 30–44 | 45 and older |
|---|---|---|---|
| Body weight | −1.80 kg ★ | −1.47 kg ★ | −2.16 kg ★ |
| Fat mass | −1.09 kg ★ | −1.22 kg (p=0.07, NS) | −1.49 kg ★ |
| Lean mass (FFM) | −0.98 kg ★ | −0.60 kg (NS) | −0.98 kg ★ |
| LDL-C | +6.75 mg/dL ★ | +1.44 mg/dL (NS) | +1.09 mg/dL ★† |
| Triglycerides | −2.69 mg/dL (NS) | +1.86 mg/dL (NS) | −7.83 mg/dL ★ |
| Fasting insulin | ↓ ★ | ↓ NS | −3.15 µIU/mL ★ |
| HOMA-IR | −0.48 ★ | −0.02 (NS) | −0.83 (p=0.07, NS) |
| Systolic BP | −2.07 mmHg (NS) | −1.52 mmHg (NS) | −4.86 mmHg ★ |
★ = p < 0.05 in standard analysis. † = significant only in conservative sensitivity analysis (r = 0.5). 1
Three patterns stand out:
Young adults (under 30) get the strongest insulin-sensitivity signal — significant reductions in fasting insulin and HOMA-IR — along with solid weight and fat loss. But they also carry the most pronounced LDL-C elevation in the dataset, at +6.75 mg/dL. For a 25-year-old whose baseline LDL-C is already at the upper end of normal, that increment is not trivial.
Early middle-aged adults (30–44) show the most attenuated response. Weight loss is statistically significant but modest (−1.47 kg), and no cardiometabolic marker — lipids, glucose, blood pressure — improves significantly. The authors suggest occupational stress, elevated cortisol, and patterns of compensatory eating may blunt the metabolic response in this cohort, though that is inference from discussion, not a tested mechanism. 1
Adults 45 and older get the best weight-loss result (−2.16 kg, the largest of the three cohorts), the only statistically significant triglyceride reduction (−7.83 mg/dL), and the only significant systolic blood pressure reduction (−4.86 mmHg). Those are meaningful cardiovascular signals. The complications, however, are also concentrated here — and are addressed next.
The two risks that appear regardless of age
LDL-C rises in every age group
The most counter-intuitive finding in the paper is that LDL-C does not fall during IF — it rises, in both young adults (significantly) and older adults (significantly once the conservative analysis is applied). Both TRF and IER (alternate-day fasting and 5:2 protocols) produced LDL-C elevations with no statistically significant difference between them (TRF: +2.30 mg/dL, IER: +1.15 mg/dL, p-interaction = 0.28). 1
The authors describe this as a "generalized physiological response to fasting interventions rather than being specific to a single modality." The proposed mechanism for younger adults involves a hepatic rebound effect — efficient fat mobilization during the fast, followed by compensatory VLDL secretion during the eating window, particularly if refeeding includes high-glycemic carbohydrates or saturated fat. In older adults, the unmasked elevation aligns with age-related decline in hepatic LDL receptor expression and diminished lipid clearance. Neither mechanism has been experimentally confirmed in these trials; the authors flag both as hypotheses.
The practical implication is stated plainly by the authors: "regardless of age, IF implementation must prioritize dietary quality during eating windows and mandate regular lipid monitoring to mitigate latent cardiometabolic risks." 1
Lean mass loss is a generalized response, not a side effect of poor protocol design
Significant fat-free mass loss appeared in adults under 30 (−0.98 kg, p = 0.020) and adults 45 and older (−0.98 kg, p < 0.001). The 30–44 cohort showed lean mass loss of −0.60 kg that did not reach significance.
Both TRF and IER produced statistically equivalent lean mass reductions (TRF: −0.96 kg, IER: −1.39 kg, p-interaction = 0.080). As the authors write, "the risk of muscle mass depletion is a generalized response to intermittent fasting, irrespective of whether the caloric restriction is daily or periodic." 1
This matters most in the ≥45 cohort because adults in that age range are already entering the window where sarcopenia — age-related muscle loss — accelerates. Losing nearly 1 kg of lean mass while also losing 2.16 kg of body weight means a meaningful fraction of the weight lost is not fat. The clinical significance depends on baseline muscle mass, but the authors describe the lean mass effect in older adults as a "severe clinical hazard" and call for a specific mitigation strategy.
Limitations
The authors are careful about the boundaries of what their data support.
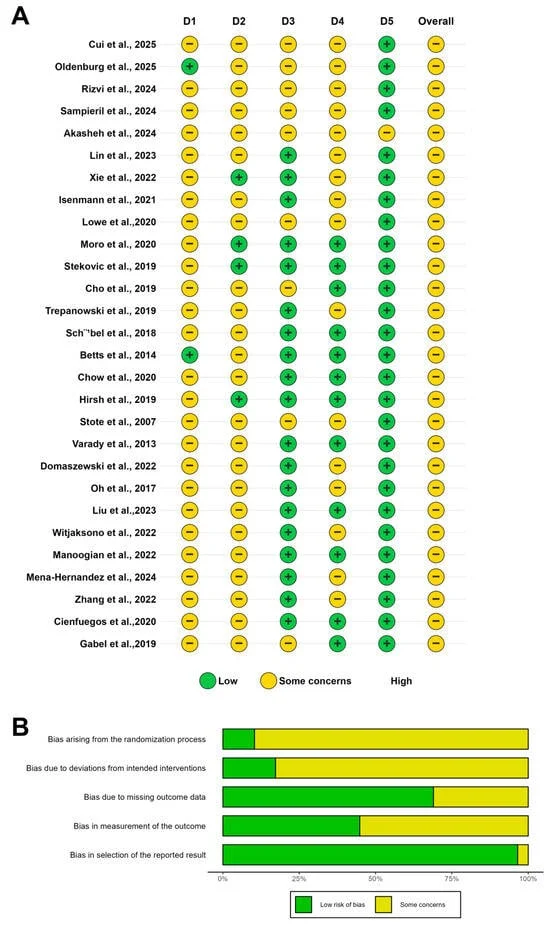
GRADE certainty is low to very low across all outcomes and all age groups. Dietary trials cannot blind participants to whether they are fasting, which introduces inherent performance bias. The majority of included studies were rated "some concerns" on overall risk of bias using the Cochrane RoB 2 tool. 1 The authors state explicitly that their findings "should not be interpreted as definitive clinical directives."
Age stratification relies on study-level mean age, not individual participant data. A study with a mean age of 40 could include participants aged 25–55. The age-group comparisons carry a risk of ecological fallacy — differences between strata may not correspond to differences between individuals of those ages within a single trial.
Multiple outcomes showed statistical fragility. Leave-one-out sensitivity analyses found that removing specific heavily-weighted trials shifted significance for several outcomes in the ≥45 cohort, including glycemic markers. Results for blood glucose and HOMA-IR in older adults should be treated with particular caution.
No sex-disaggregated data were available. The vast majority of included trials enrolled mixed-sex cohorts without reporting outcomes separately by sex. The authors note that "given the well-established dimorphism in regional fat deposition and hormonal regulation (e.g., the protective metabolic effects of estrogen in premenopausal women), it is highly probable that male and female bodies adapt differently to IF." That question cannot be answered from this dataset. 1
Participants were healthy or overweight/obese only. Results cannot be extrapolated to people with type 2 diabetes, cardiovascular disease, metabolic syndrome, or other cardiometabolic comorbidities. For those populations, IF protocols require clinical supervision that falls outside the scope of this meta-analysis.
Trial durations were short. The range of 4 weeks to 12 months does not tell us what happens after year one — whether the LDL-C elevation persists, whether lean mass loss plateaus, or whether the blood pressure and triglyceride benefits in older adults are durable.
Dietary recommendation
IF remains a legitimate weight-management tool for healthy adults. This meta-analysis does not argue against using it. What the data do argue is that the protocol should be tailored by age, and that two specific safety checkpoints apply to everyone who uses IF regardless of which format they choose.
For adults under 30: IF produces the strongest insulin-sensitivity signal and solid fat loss, but LDL-C elevation is the most pronounced in this cohort (+6.75 mg/dL on average). If you start IF at this age, get a fasting lipid panel before starting and recheck at 8–12 weeks. If your LDL-C rises more than 10–15 mg/dL from your personal baseline, revisit your eating-window food quality — especially your intake of saturated fat and high-glycemic carbohydrates during refeeding.
For adults 30–44: Expect modest weight loss and minimal cardiometabolic improvement from standard IF. If your primary goal is metabolic improvement rather than weight management, the evidence from this meta-analysis suggests IF alone is likely insufficient for this age group. A dietary approach with stronger metabolic evidence (whole-food Mediterranean pattern, reduced refined carbohydrate intake) may produce more reliable cardiometabolic results. If you continue IF, lipid monitoring still applies.
For adults 45 and older: The cardiometabolic benefits are the most robust in this group — significant triglyceride reduction (−7.83 mg/dL) and systolic blood pressure reduction (−4.86 mmHg) — but so is the lean-mass risk. Xing et al. advocate what they call an "IF+" strategy: daily protein intake of ≥1.2–1.5 g/kg body weight, resistance training targeting large muscle groups 2–3 times per week, and body composition monitoring beyond simple scale weight (ideally DXA, or at minimum tracking waist circumference alongside weight). 1 The standard IF protocol without protein and resistance support in this age group converts some of the weight loss from fat into lean tissue — which may exchange one risk for another.
For everyone: Monitor LDL-C. The finding that LDL-C rises across both major IF modalities — TRF and IER — with no significant difference between them means there is no protocol switch that avoids this signal. Eating-window food quality matters: the proposed mechanism involves compensatory lipid secretion during refeeding, which is plausibly worsened by high-saturated-fat or high-glycemic refeeding meals. Prioritizing protein, fiber, and unsaturated fats during eating windows is the practical countermeasure the evidence currently supports.
Cover image: AI-generated editorial illustration.
이 콘텐츠를 둘러싼 관점이나 맥락을 계속 보강해 보세요.